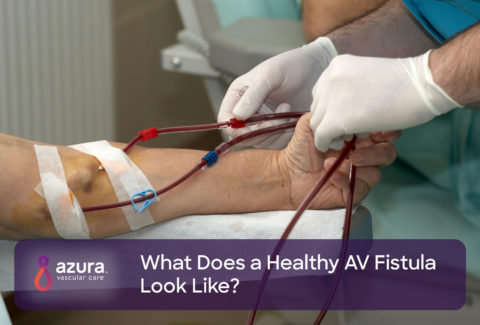
Following the creation of a vascular access, keeping it well-functioning is necessary to ensure successful dialysis treatments. For hemodialysis patients, aneurysms and pseudoaneurysms are associated with arteriovenous (AV) fistulas and grafts. They can be common and result in serious complications. Studies show that aneurysms occur in between 5% and more than 60% of patients with AV fistulas and grafts. (1)
True Aneurysm vs Pseudoaneurysm: What is the Difference?
What is a True Aneurysm?
In general, an aneurysm is a weak spot in the wall of your access that can expand and eventually burst if not treated. In a true aneurysm, the artery or vessel dilates in response to the increased blood flow, sometimes causing a blood-filled sac to form.
What is a Pseudoaneurysm?
A pseudoaneurysm, or a “false aneurysm” occurs when a blood vessel wall or the graft wall is injured, and the blood is contained by the surrounding tissues. A pseudoaneurysm typically occurs from trauma, such as repetitive needle sticking in the same location, resulting in blood leaking out of the access and into the surrounding tissue.
Aneurysms most often occur in an AV fistula and pseudoaneurysms are more common in AV grafts. However, either type of aneurysm can occur in both types of access.
What Are the Symptoms of an Aneurysm or Pseudoaneurysm?
Aneurysms and pseudoaneurysms occur when the vein or artery used to create the fistula or graft starts to weaken or is damaged. Keep in mind that this complication is considered relatively common. Thus, it’s important that you know the symptoms of both aneurysms and pseudoaneurysms, so you can be on the lookout and detect them early on.
Symptoms of aneurysms and pseudoaneurysms are similar and can include one or more of the following:
- Localized enlargement of the vein which is visible to the eye and may progressively grow larger.
- Increased blood flow through the fistula or graft
- Thinning of the skin over the fistula or graft
- A shiny appearance of the skin over the fistula or graft
- Pain
What Causes an Aneurysm or Pseudoaneurysm?
Aneurysms and pseudoaneurysms usually develop over time.
- They tend to develop at the site of multiple needle sticks
- Due to the high blood flow through the fistula or graft, the involved blood vessel may enlarge and expand, predisposing it to an aneurysm or pseudoaneurysm
Treatment for An Aneurysm vs Pseudoaneurysm
Treatment for Aneurysms
Not all aneurysms require treatment. Small, stable aneurysms typically have thick walls and can be monitored to make sure they don’t become larger.
You should, however, be concerned about aneurysms that show one or more the following signs:
- Rapid increase in size
- Pain
- Thinning of the skin
- Shiny and pulsating
- Infection (2)
These are all signs that an aneurysm may rupture. A rupture may occur underneath the skin, or it can break through the skin. A ruptured aneurysm or an aneurysm that is about to rupture is considered an emergency. First, the bleeding must be stopped. Once the bleeding is stopped, the AV fistula can be properly assessed. Sometimes, the fistula can be reconstructed or repaired.
Even though repair is sometimes possible, it’s best to try to save a fistula before the aneurysm progresses to the point of rupture. With small aneurysms, if necessary, the AV fistula can be reconstructed before a rupture occurs.
A stent can be placed inside the blood vessel with the aneurysm, but this can compromise the fistula, making needle sticks more difficult. (1) This option is often reserved for patients who are not healthy enough to undergo surgery, or as a temporary measure before AV fistula reconstruction can be done.
Treatment for Pseudoaneurysms
The management of pseudoaneurysms is similar to the treatment for aneurysms.
However, small pseudoaneurysms with narrow necks can sometimes can be treated with an injection of thrombin, a drug used to control minor bleeding, or with ultrasound compression (1, 3, 4).
Large pseudoaneurysms, and those that do not resolve using thrombin injections or ultrasound compression may require surgical repair. Surgical intervention is done to prevent further enlargement and other complications, such as rupture. (2)
Pseudoaneurysms that result from infection, which is more common with AV grafts than AV fistulas, almost always require surgery. The surgery for these pseudoaneurysms is more extensive than other repairs, and the chance of rupture is high. (2)In general, if the pseudoaneurysm is the result of an infection, the graft should be ligated (tied off) and possibly removed.
Aneurysms and pseudoaneurysms are not uncommon complications for patients with AV fistulas or AV grafts. Knowing the early warning signs and symptoms and understanding the treatment options for these complications is key in treating them and salvaging the access.
Sources:
i Clark, T.W., and Abraham, R.J. (2000). Thrombin injection for treatment of brachial artery pseudoaneurysm at the site of a hemodialysis fistula: report of two patients. Cardiovasc Intervent Radiol, 23: 396–400
ii Mudoni, A., Cornacchiari, M., Gallieni, M., Guastoni, C, McGrogan, D, Logias, F., Ferramosca, E., Mereghetti, M., and Inston, N. (2015) Aneurysms and pseudoaneurysms in dialysis access, Clin Kidney J (2015) 8 (4): 363-367.
iii O’Neill, J.M., and Jenkins, D.A. (2001). Ireland HM Recurrence of dialysis shunt pseudoaneurysm following percutaneous thrombin embolization, Cardiovasc Intervent Radiol, 24: 441–442
iv Witz, M., Werner, M, Bernheim, J., et al. (2000). Ultrasound-guided compression repair of pseudoaneurysms complicating a forearm dialysis arteriovenous fistula. Nephrol Dial Transplant, 15: 1453-1454